Chapter 28 Diuretic Drugs
Carbonic anhydrase inhibitors
Acetazolamide
CAIs block the action of carbonic anhydrase, thus preventing the exchange of H+ ions with sodium and water.
• Long term management of open angle glaucoma,
• Edema,
• High-altitude sickness,
• Used with miotics to lower intra-ocular pressure before ocular surgery.
Contraindicative:
Known drug allergy
Hyponatremia
Hypokalemia
Severe renal or hepatic dysfunction
Adrenal gland insufficiency
Cirrhosis
Adverse effects:
Acidosis
Hypokalemia
Drowsiness
Anorexia
Paresthesias
Hematuria
Urticaria
Photosensitivity
Melena (blood in the stool)
Interactions:
• Because CAIs can cause hypokalemia, an increase in digoxin toxicity may occur when they are combined with digoxin.
• Use with corticosteroids may also cause hypokalemia.
• Increased effects of amphetamines, carbamazepine, cyclosporine, phenytoin, and quinidine with concurrent use of CAIs
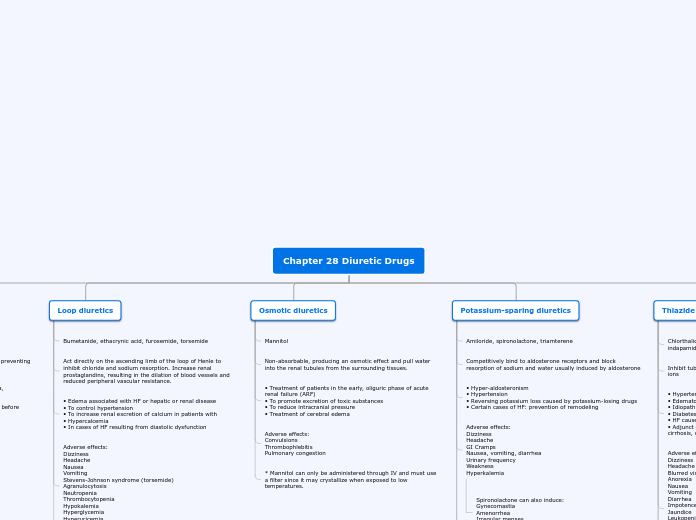
Loop diuretics
Bumetanide, ethacrynic acid, furosemide, torsemide
Act directly on the ascending limb of the loop of Henle to inhibit chloride and sodium resorption. Increase renal prostaglandins, resulting in the dilation of blood vessels and reduced peripheral vascular resistance.
• Edema associated with HF or hepatic or renal disease
• To control hypertension
• To increase renal excretion of calcium in patients with
• Hypercalcemia
• In cases of HF resulting from diastolic dysfunction
Adverse effects:
Dizziness
Headache
Nausea
Vomiting
Stevens-Johnson syndrome (torsemide)
Agranulocytosis
Neutropenia
Thrombocytopenia
Hypokalemia
Hyperglycemia
Hyperuricemia
Photosensitivity
Interactions:
• Neurotoxic
• Nephrotoxic
• Increase serum levels of uric acid, glucose, alanine aminotransferase, and aspartate aminotransferase.
Osmotic diuretics
Mannitol
Non-absorbable, producing an osmotic effect and pull water into the renal tubules from the surrounding tissues.
• Treatment of patients in the early, oliguric phase of acute renal failure (ARF)
• To promote excretion of toxic substances
• To reduce intracranial pressure
• Treatment of cerebral edema
Adverse effects:
Convulsions
Thrombophlebitis
Pulmonary congestion
* Mannitol can only be administered through IV and must use a filter since it may crystallize when exposed to low temperatures.
Potassium-sparing diuretics
Amiloride, spironolactone, triamterene
Competitively bind to aldosterone receptors and block resorption of sodium and water usually induced by aldosterone
• Hyper-aldosteronism
• Hypertension
• Reversing potassium loss caused by potassium-losing drugs
• Certain cases of HF: prevention of remodeling
Adverse effects:
Dizziness
Headache
GI Cramps
Nausea, vomiting, diarrhea
Urinary frequency
Weakness
Hyperkalemia
Spironolactone can also induce:
Gynecomastia
Amenorrhea
Irregular menses
Postmenopausal bleeding
Interactions:
Lithium-lithium toxicity
Angiotensin-converting enzyme inhibitors-hyperkalemia
Potassium supplements-hyperkalemia
NSAIDs-decrease diuretic effect
*Amiloride is less effective in the long term
Thiazide and thiazide-like diuretics
Chlorthalidone, chlorothiazide, hydrochlorothiazide, indapamide, metolazone
Inhibit tubular resorption of sodium, chloride, and potassium ions
• Hypertension
• Edematous states
• Idiopathic hypercalciuria
• Diabetes insipidus
• HF caused by diastolic dysfunction
• Adjunct drugs in treatment of edema related to HF, hepatic cirrhosis, or corticosteroid or estrogen therapy
Adverse effects:
Dizziness
Headache
Blurred vision
Anorexia
Nausea
Vomiting
Diarrhea
Impotence
Jaundice
Leukopenia
Agranulocytosis
Urticaria
Photosensitivity
Hypokalemia
Hyperglycemia
Hyperuricemia
Hypochloremic alkalosis
Interactions:
Anti-diabetic drugs-reduced therapeutic hypoglycemic effect
Corticosteroids-hypokalemia
Digoxin-digoxin toxicity
Lithium-lithium toxicity
NSAIDs-decreased diuretic activity
* Thiazide should not be used if creatine is <30-50 mL/min
* Metolazone remains effective even if creatine is 10 mL/min