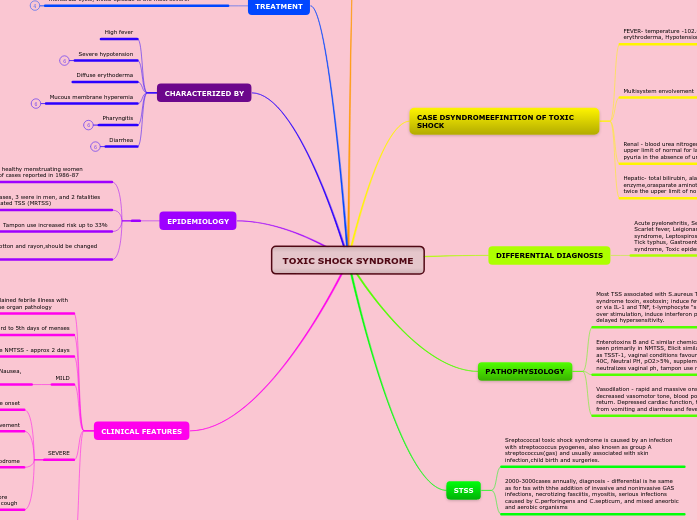
TOXIC SHOCK SYNDROME
INTRODUCTION
MUSCULAR -sever myalgia or creatine phosphokinase level at least twice the upper limit of normal
Discovered in 1978 in apparently healthy children- staph aureus isolated
TSS epidemic- 1981 associated with increased tampon use
CASE DSYNDROMEEFINITION OF TOXIC SHOCK
FEVER- temperature -102.0F , rash-diffuse macular erythroderma, Hypotension
Multisystem envolvement
GI- vomiting or diarrhea at onset of illness
Muscular -serve myalgia or creatine phosphokinaselevel at least twice the upper limit of normal
Mucous membrane - vaginal, oropharyngeal, or conjunctival hypermia
Renal - blood urea nitrogen or ceatinine at least twice the upper limit of normal for laboratory or urinary sediment with pyuria in the absence of urinary tract infection
Hepatic- total bilirubin, alanine aminotransferase enzyme,orasparate aminotransferase enzyme levels at least twice the upper limit of normal for laboratory.
DIFFERENTIAL DIAGNOSIS
Acute pyelonehritis, Septic shock, Acute rheumatic fever, Scarlet fever, Leigionare's disease, PID, HUS, Acute viral syndrome, Leptospirosis, SLE, Rocky mountain spotted fever, Tick typhus, Gastroenteritis, Kawasaki disease, Reye syndrome, Toxic epidermic necrolysis, Erythema multiforme
PATHOPHYSIOLOGY
Most TSS associated with S.aureus TSST-1; toxic shock syndrome toxin, exotoxin; induce fever via the hypothalamus or via IL-1 and TNF, t-lymphocyte "superantigenation" and over stimulation, induce interferon productiion, enhance delayed hypersensitivity.
Enterotoxins B and C similar chemical structure to TSST-1 seen primarily in NMTSS, Elicit similar clinical manifestations as TSST-1, vaginal conditions favourable to TSST-1, temp 39-40C, Neutral PH, pO2>5%, supplemental CO2, menstruation - neutralizes vaginal ph, tampon use may increase O2 and CO2.
Vasodilation - rapid and massive onset, hypotension, decreased vasomotor tone, blood pooling, decreased vascular return. Depressed cardiac function, total body water deficits from vomiting and diarrhea and fever.
STSS
Sreptococcal toxic shock syndrome is caused by an infection with streptococcus pyogenes, also known as group A streptococcus(gas) and usually associated with skin infection,child birth and surgeries.
2000-3000cases annually, diagnosis - differential is he same as for tss with thhe addition of invasive and noninvasive GAS infections, necrotizing fasciitis, myositis, serious infections caused by C.perforingens and C.septicum, and mixed aneorbic and aerobic organisms
TREATMENT
Aggressive shock management, Continuous monitoring: central Aggressive fluid replacement- 4-20L crystalloid and FFP, Ventilatory management if ARDS develpos complete blood work and cultures, removal of foreign bodies,i.e tampon or nasal packing, Antistaphlococcal penicilin or cephalospori. Pt not treated with beta-lactamase-stable abx can have recurrence, MRTSS - recurrence occcur in second month aftetr the innitial disease, recurring on the same day of the menstrual cycle, Initisl episode is the most severe.
CHARACTERIZED BY
High fever
Severe hypotension
Diffuse erythoderma
Mucous membrane hyperemia
Pharyngitis
Diarrhea
EPIDEMIOLOGY
TSS- a disease of young healthy menstruating women comprised fifty percent of cases reported in 1986-87
In 2000, 135 reported cases, 3 were in men, and 2 fatalities were from menstrual-related TSS (MRTSS)
Tampon use increased risk up to 33%
tampons now made of cotton and rayon,should be changed every 4-8 hours.
CLINICAL FEATURES
TSS must be considered when- unexplained febrile illness with erythroderma, hypotension, and diffuse organ pathology
Pts with NMTSS present 3rd to 5th days of menses
Postoperative NMTSS - approx 2 days
MILD
Fever, Chills, Myalgias, Abdominal pain, Sore throat, Nausea, Vomiting, Diarrhea, Self-limitng
SEVERE
Acute onset
Early multiorgan envolvement
Prodrome
Headache, malaise, myalgia, nausea, vomiting and diarrhea
Sudden onset of fevers and chills 1-4days prior to presentation
orthostatic lightheadedness, profuse watery diarrhea, sore throat, paresthesias, photophobia, abdominal pain, and cough
Focal neuro findings are rare, Varying degrees of altered consciousness, Toxic encephalopathy - confusion, disorientation, agitation, hysteria, somnolence, and seizures